
Template File: /www/wp-content/themes/stn2017/index.php | Template Hierarchy
WP version: 6.7.2
PHP version 8.2.28
The trauma course which starts where the others end
Take advantage of this rare opportunity to undertake the Trauma Care After Resuscitation (TCAR) course in-person. Unlike trauma programmes targeted at prehospital or emergency care providers, TCAR is explicitly designed for bedside professionals who care for injured patients in critical care, theatre, HDU, ward and in rehabilitation settings. It provides a sound knowledge base for patient care in the hours, days and weeks after trauma.
TCAR gives delegates the knowledge and clinical reasoning skills to address numerous NMTNG competencies. It begins by focussing on concepts relevant to the nursing care of all injured, hospitalised patients, before progressing to cover the injury-to-discharge care of trauma patients.
This is a rare opportunity to join the course in-person in Scotland, while having the chance to network with like-minded professionals from across the UK. This is especially important for staff who work in major trauma centres and trauma units in outlying wards, to further support and develop their trauma knowledge and provide a platform for meeting like-minded professionals.
For more information about the course, visit the TCAR website. The paediatric care after resuscitation (PCAR) is also available this summer in Liverpool, on 19-20 June (see attached brochure for details).
Cost: £315 per person for the 2-day course. This includes one year access to additional TCAR course content, resources, and 18 CPD hours.
How to book: Book the Glasgow course via the TCAR website.
The Scottish Trauma Network held an online learning event in October 2024, hosted by colleagues from the South East of Scotland.
The event focused on rehabilitating patients with frailty and delirium. Helen, a physiotherapist at the Major Trauma Centre in Glasgow, provided the following summary.
What it was about?
The event set out to explain what frailty and delirium is in trauma patients and aimed to upskill staff on how this can be scored, how this effects patients’ journeys through hospital and their recovery and how staff are able to help someone come out of delirium.
The event featured interesting and interactive talks about frailty and information on using the Clinical Frailty Score. This provided a level of insight into the importance of gathering good baseline information.
Additionally, therapists shared case studies of two frail patients, illustrating contrasting rehab journeys and outcomes for each patient.
What I learned?
Key takeaways included learning how to effectively use the Clinical Frailty Score, understanding its implications for rehabilitation and recovery, and incorporating this knowledge into rehab planning and goal setting.
What I’ll take from it?
The event improved my understanding of the Clinical Frailty Score and emphasised the value of considering patients’ backgrounds and recovery expectations to enhance communication and referrals for DME and slow-stream recovery programs.
Overall, the event was both insightful and engaging, with knowledgeable speakers delivering charismatic and interactive presentations. The lessons learned will inform clinical practice and patient care moving forward.
University Hospital Wishaw (UHW) was identified as a STAG mortality outlier for 2017 – 2019 inclusive.
As a result, a high-level multidisciplinary mortality review process of all trauma deaths was conducted. This is now established as an essential part of the UHW Major Trauma annual clinical governance process.
These annual mortality reviews identified three key areas for quality improvement initiatives due to the excess mortality demonstrated:
The quality improvement initiatives commenced during 2021 and coincided with the employment of the NHS Lanarkshire Major Trauma Coordinator who has driven them forward. The projects were supported by an extensive education programme for medical, nursing and AHP staff as well as continued ward support.
These interventions have led to significant improvements in mortality in both patient groups,
It is highly encouraging that in the STAG 2024 Annual Report, UHW were no longer Scottish mortality outliers for 2021 – 2023 inclusive. This sustained improvement in mortality demonstrated the case for an additional Major Trauma Coordinator to allow expansion of the service.
What is it?
HECTOR began as the Heartlands Elderly Care Trauma and Ongoing Recovery course that was established to develop a training programme for clinicians and practitioners who are responsible for looking after older people who have injuries.
These injuries that an individual sustains often play second fiddle to the complex comorbidities, frailty, and the challenges of caring for them within an ever-pressured emergency care system.
This course is a two day course covering the assessment and management of elderly patients involved in trauma, and their first 48-72 hours in hospital. The course takes a mixed approach to education – with lectures, discussion groups and practical moulage stations. As a participant you’d be involved in all of these areas and would be split into mixed specialty/discipline groups for the small group work.
Who is it for?
Healthcare professionals working with elderly people in the first 24-72 hours after sustaining traumatic injury either as part of the initial assessment or the early stages of rehabilitation.
Previous course participants have included advanced physiotherapists, occupational therapists, consultants and registrars in emergency medicine, geriatric medicine, general surgery and orthopaedics; general practitioners and prehospital responders; major trauma coordinators; nurses working with trauma patients; paramedics and rehabilitation staff.
Who is running it?
An interspecialty and multidisciplinary faculty from the Scottish (STN) and Northern Trauma Network England (NTN). The NTN have kindly supported the setting up of this course.
When is it?
There will be selected dates across the year – however if you apply (see below) then you will be informed when you are at the top of the waiting list, of when the next courses are available.
How do I apply?
Click this link or scan the QR code: HECTOR Application Form
If the link doesn’t work, then please email fv.hectorcourse@nhs.scot for an application form.

Cost:
£350 for doctors, £200 for NMAHPs.
The difference in price is based on availability of study budgets for non-mandatory courses between staff groups.
Any questions, then email the centre fv.hectorcourse@nhs.scot
Many thanks,
Joel, Claire, Jon and Sarah (HECTOR Scotland faculty)
![]()
![]()

![]()
The Scottish Trauma Network (STN) are pleased to announce the Healthcare Support Worker (HCSW) Nursing, Midwifery and Allied Health Professions (NMAHP) Development Framework for Major Trauma is now published.
The framework is hosted on the STN website and can be found at the link below
https://scottishtraumanetwork.com/our-work/education-learning/
The framework will be used by HCSW NMAHP practitioners caring for major trauma patients in any in-hospital in for identifying, planning and supporting learning needs, identifying career pathways and enhancing workforce planning.
This framework is the result of collaborative working between NHS Education for Scotland (NES) and the STN, working closely with HCSW NMAHP practitioners and consulting with the STN Education and Workforce group. It provides specialist content and is a “bolt-on” to the already published NES HCSW NMAHP Education and Development Framework which should be referred to first for detail of four pillars of practice, guidance on how to use the framework and information on accountability and delegation.
This completes the STN’s objective of having a development framework for all NMAHP roles in major trauma. Next steps are to strengthen implementation and gather feedback.
The first Scottish cohort of the silver trauma course HECTOR was delivered at Scottish Centre for Simulation and Clinical Human Factors (SCSCHF) on the 20th and 21st March.
The 15 participants were from mixed professions including care of the elderly and frailty medicine, GPs, advanced practitioners from nursing and allied health professions and major trauma co-ordinators. All the Scottish regional trauma networks were represented
The Hector faculty from the Northern Trauma Network in England travelled to Scotland to facilitate the programme alongside Dr Joel Burton and other STN colleagues.
It was a busy 2 days filled with simulated scenarios to practice assessment and decision-making skills with supportive materials and discussion.
There was lots of positive energy and initial feedback from the participants was that they valued the course content, approach and learning from each other. Next steps are formal evaluation and to grow the Scottish faculty for the next cohort
![]() .
.![]()
![]()

Chelsey Smith was 15 when she was left with life-threatening injuries, following a road traffic accident in February last year.
After an initial assessment at the University Hospital in Wishaw, Lanarkshire, Chelsey was rushed to the West of Scotland’s Paediatric Major Trauma Centre in Glasgow for specialist treatment.
Consultant Paediatric Neurosurgeon Roddy O’Kane performed the surgery, to reduce the swelling and pressure on Chelsey’s brain, with part of her skull being removed and stored in her stomach to keep it sterile.
Following intensive rehab with the team at the RHC, Chelsey, who is now 16, has made a remarkable recovery and, less than a year after her final surgery, was a guest of honour at the Major Trauma Centre’s training day this week.
She said: “I just can’t thank all of the team here at the Royal Hospital for Children in Glasgow for everything they have done for me, they have saved my life and given me my life back too.
“I don’t remember much about the day of the accident to be honest, but I’m here now and that’s what matters. I have had so much support from Roddy, my Major Trauma Co-ordinator Lynsay Stewart, all of the staff at the hospital and of course my family.
“Roddy was able to magically take a part of my skull and put it in my stomach to let the swelling reduce in my brain, I don’t really know how it works but it’s amazing. It was a long journey and I would tell anyone who is in a similar situation to keep going, to make this recovery you have to be mentally prepared for it too and thankfully I had so many positive people around me to help with that.”
Chelsey is now back preparing for her exams at Brannock High in Newarthill, has been able to get a part-time job and is hoping to go on to study accountancy.
She said: “Obviously everything that happened was not good, but thanks to the Royal Hospital for Children team in Glasgow I have been able to get back to school and have also started a part-time job.
“I just want to say thank you again to everyone for all they have done for me. Even after my follow-up appointments are finished, I’ll keep coming back to visit, I have missed them all.”
The procedure which involves removing part of the skull is not common, but after other medical interventions were unsuccessful it was the last option to save Chelsey’s life.
Roddy said: “This procedure is not something that we do every day but it gave Chelsey the best chance of surviving the injuries she had sustained during the accident.
“We take part of the skull out and store it in the stomach in order to keep it sterile, this is usually re-attached after a couple of months once swelling has reduced.
“Chelsey’s recovery is absolutely remarkable, based on her condition when she arrived it is incredible to see how well she is doing. There was a real danger to her life and we also anticipated that there would be more of lasting impact on her life.
“We are all so proud of Chelsey and all of the hard work she has put in during her rehab with our specialist teams. We’re delighted for her and her family and were all beaming from ear to ear when we got to see her again today.”
The development of the Major Trauma Service in the West of Scotland came with significant resource to provide rehabilitation in order to achieve the Scottish Trauma Networks stated aim of: Saving Lives. Giving Life Back.
The rehabilitation team within the Major Trauma ward in the Queen Elizabeth University Hospital are delivering early, intensive, multidisciplinary rehabilitation to patients who are multiply injured and have complex rehabilitation needs. The team consists of speech and language therapists, physiotherapists, occupational therapists, clinical psychologists, dietitians, therapy support workers and major trauma co-ordinators.
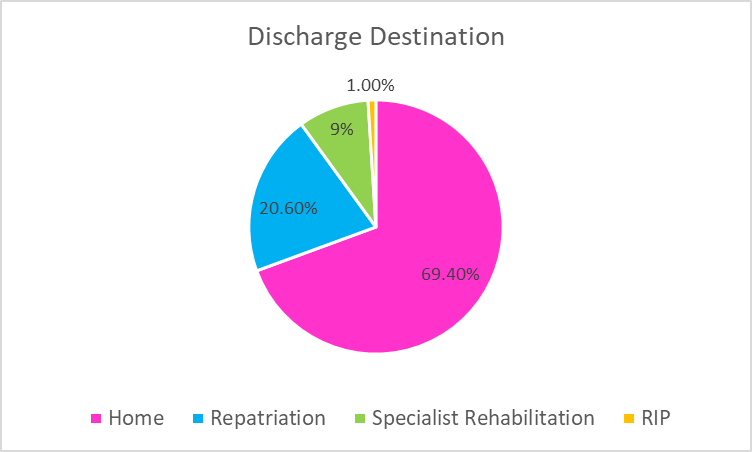
Initial results are extremely positive and a number of QI projects have also been carried out. An analysis of the data collated since the Major Trauma ward opened in August 2021 shows that the median length of stay in the ward is 10 days. It also showed that 69.4% of patients were discharged straight home from the ward and 20.6% required repatriation to their local hospital. This has contributed to an improved patient journey and in these times of significant pressure on the NHS, is reducing the requirement for ambulance transfers and beds in trauma units.
“a set of measures that assist individuals, who experience or are likely to experience disability, to achieve and maintain optimum functioning in interaction with their environments”
(WHO, 2011)
Evidence shows that the earlier rehabilitation is provided and the greater the intensity, the better the outcomes for the patient (Hartley, Keevil, Alushi et al, 2019). It was with this evidence in mind that the ethos of the STN was developed.
The rehabilitation needs of medical inpatients is changing. Development of community based, admission avoidance schemes means that patients admitted to hospital tend to be more unwell and have more complex rehabilitation needs. This has been exacerbated by the COVID-19 pandemic: patients are more frail, deconditioned, present later in disease course and a significant proportion have underlying neurological diagnosis.
Ongoing challenges around bed capacity and ‘front door’ performance forced the opening of additional medical beds in the QEUH in October 2021. The current staffing complement within the medical sector is not able to meet the rehabilitation needs of the patients (Staff to patient ratios: Physiotherapy (PT) = 1:41, Occupational therapy (OT) = 1:56). This means that patients who are assessed as requiring rehabilitation, are seen on average twice a week.
Current staffing resource within the AHP team does not meet the rehabilitation needs of the patients who are located within medical, resulting in longer lengths of stay and reduced independence on discharge requiring significant packages of care and equipment provision. This has financial implications for the NHS in terms of bed days and equipment provision, and for Social Care in terms of ongoing provision of support at home, in addition to the detrimental effects for patients who they are not being facilitated to achieve their maximal functional potential.
Ward 11D was turned fully into a medical ward in October 2021. As no additional AHP staff were provided for these additional bed numbers, and with medical AHP staffing numbers already being low, the AHP Team from the Major Trauma ward were asked to cover these additional medical beds.
This situation was used as an opportunity to collect data on what therapy input and therapy resource was required by the patients within this area to ensure the best quality of care was provided to patient and service and assess the impact of enhanced staffing levels on patient length of stay and outcome.
PT and OT staff from the Major Trauma ward team were assigned to cover the additional medical beds, these staff had experience in neurorehabilitation and were a mix of bands from 6 to 8B.
Increased staff to patient ratio was made available compared to ‘normal’ staffing levels on established general medical wards.
All patients referred to PT/OT over a 6 week period were included.
Patients were provided with daily therapy input as required.
Rehabilitation need and complexity were quantified using the standardised Rehabilitation Complexity Scale (RCS-E)
Data on number of referrals, diagnosis, reason for admission, number of treatment sessions, hours of treatment and number of therapists required for each treatment session was collected in addition to length of stay, and requirement for onward referral to community teams or for packages of care at point of discharge.
Data was collected from both the intervention ward (with enhanced AHP staffing levels) and a comparator ward (with ‘normal’ medical AHP staffing).
The data gathered from both areas is summarised in the following table:
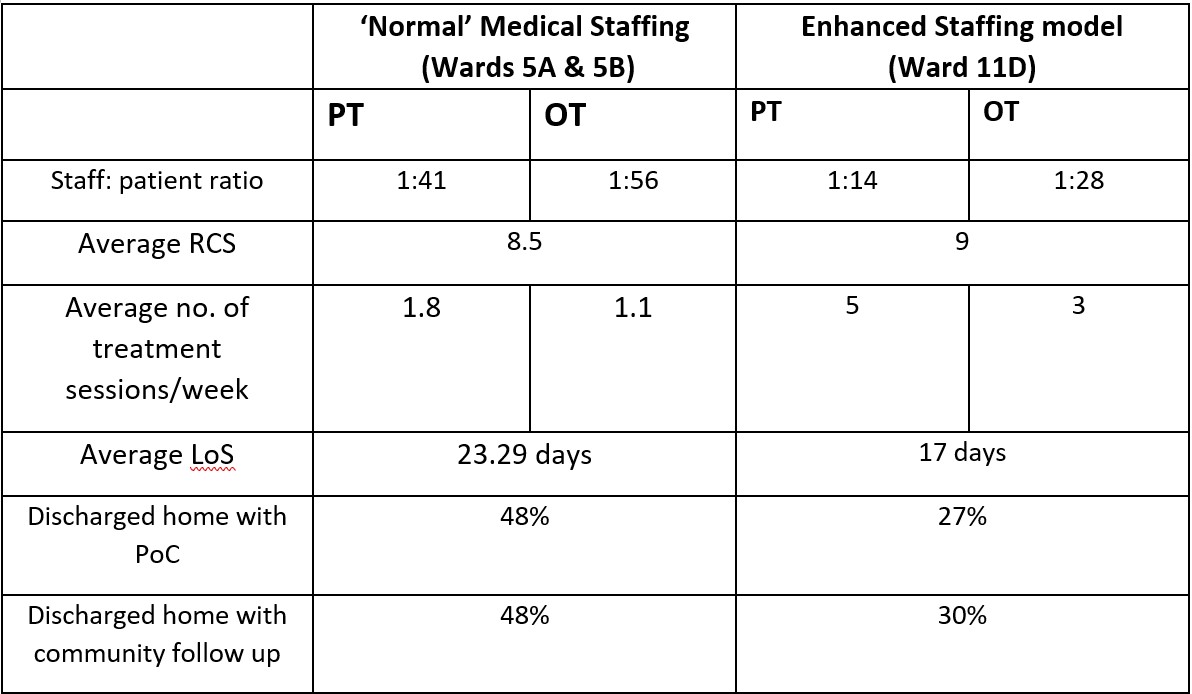
Specific case studies and anecdotal evidence from the Major Trauma team’s time covering 11D showed that it was not only the number of staff available to treat patients that had a positive impact on LOS and patient outcomes. They also found that having staff who were knowledgeable and had experience treating patients with neurological diagnosis with complex rehabilitation needs, was beneficial.
The data highlights that the right number of staff and experience has a significant impact on reducing patients LOS and improving patient outcomes. In this audit LOS was reduced by 6.29days and less patients were referred onto community rehabilitation teams therefore suggesting they achieved their rehabilitation potential in hospital as they received the right amount of specialist treatment. Additionally, significantly fewer packages of care were required for the patients discharged home. This evidence suggests that early and adequate provision of OT/PT intervention is beneficial not only for patients but also for the hospital.
Overall, the data gathered supports the conclusion that improved PT and OT staffing levels can have a positive impact on length of stay and patient outcomes for patients with complex rehabilitation needs, currently managed within medical wards. Ultimately this could result in reduced spend on bed days, equipment provision and care needs for these patients.
The planning and finance department calculated that based on the proposed figure of 416 patients being discharged each year, with an average reduction in length of stay of 6 days per patient, this could potentially save 2496 bed days per year. Based on a cost of £1,200 per day for a general medical bed, this would equate to a saving of £2,995,200 for bed days.

Implementation of the Major Trauma service in the West of Scotland came with significant allocation of resource for rehabilitation. This is to provide early, intensive rehabilitation in line with the British Society for Rehabilitation Guidelines (BSRM, 2015) in order to meet the networks aim of ‘Giving Life Back’.
There is a growing body of evidence which links at least daily multidisciplinary rehabilitation provision with an improvement in long term functional ability (Fan et al, 2020), particularly in patients following acquired brain injury (Konigs et al, 2018).
For patients not on the Major Trauma pathway, this level of daily intervention is not possible due to limited AHP and clinical/neuropsychology rehabilitation resource within the acute neurosurgical service at the Institute of Neurological Sciences (INS). The project compares the rehab provision in INS to major trauma who are staffed at an appropriate level.
Aims
Six patients with a diagnosis of brain injury who did not follow the MT pathway were identified and compared with six patients with similar demographics and initial presentation who followed the MT pathway.
Patients were highlighted for the comparison project by the Head Injury Advanced Practitioners at the QEUH.
Outcome measures used: Rehabilitation Complexity Scale (RCS) and the Functional Independence Measure + Functional Assessment Measure (FIM+FAM).
Data was collected on length of stay, disciplines involved, therapy attendances/hours and discharge destination.
Although a small sample size it highlights the variation for patients with similar presentations.
Outcome measures: Improvement in both outcome measures with average FIM+FAM score increasing (by 94 compared to 49) and RCS score decreasing (-9 compared to -5) for MT patients.
In addition to the significantly better patient outcomes on the major trauma pathway it also highlights:
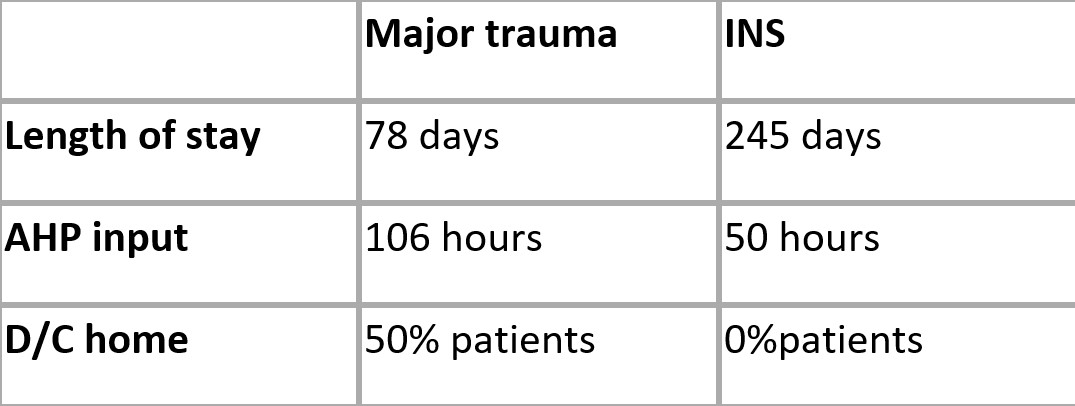
The results of preliminary examination appear to support the hypothesis that patients following the MT pathway, who receive early, intensive, daily input from a multidisciplinary team, have a reduced length of stay and improved functional outcomes compared with those who are not on the MT pathway.
Ongoing research in conjunction with INS colleagues is indicated to yield a larger sample size and determine the reliability of these results and the associated cost savings in relation to bed days in an inpatient bed and long term care needs.
In addition to the findings from the two pilot projects completed, an analysis of the data collated since the Major Trauma ward opened in August 2021 shows that the median length of stay in the ward is 10 days.
It also showed that 69.4% of patients were discharged straight home from the ward and 20.6% required repatriation to their local hospital. This has contributed to an improved patient journey and in these times of significant pressure on the NHS, is reducing the requirement for ambulance transfers and beds in trauma units.
Of the patients that were discharged home, only 24% of them required onward referral for community follow up (Community Rehab Teams, MSK services, Brain injury Teams). Additionally only 6% of patients required a Package of Care at point of discharge.
These results are further evidence that having adequate rehabilitation resource which allows early, specialist multi-disciplinary rehabilitation to be carried out result in shorter length of stay, improved patient flow, improved patient outcomes and a reduction in the requirement for packages of care and community rehabilitation on discharge. The provision of this resource is therefore a benefit to both major trauma patients and the service.
The Scottish Trauma Network (STN) are pleased to announce the publication of the Nursing, Midwifery and Allied Health Professions (NMAHP) NMAHP Development Framework for Major Trauma.
This is hosted within the Education and Training section of the STN website;
https://www.scottishtraumanetwork.com/our-work/education-learning/
The NMAHP Development Framework for Major Trauma will be used by NMAHP practitioners caring for major trauma patients in any in-hospital setting at local, regional and national levels for identifying, planning and supporting learning needs, identifying career pathways and enhancing workforce planning.
This framework is the result of collaborative working between NHS Education for Scotland (NES) and the STN, working closely with NMAHP practitioners and consulting with the STN Education and Workforce group. It is aligned to the already published NES NMAHP Development Framework.
It is currently for registered practitioners at education levels 5-8 with the Healthcare Support Worker element following later in the year, in conjunction with the national HCSW commission.